 Locations
Locations


Robotic Joint Replacement
Joint replacement operations have an excellent success rate with patient who were previously crippled by painful, stiff, arthritic joints able to walk again. During the operation the surgeon cuts and prepares the bone then places the new prosthesis as accurately as possible in position using a series of jigs, saws and other instruments. Our aim is always to be as accurate as possible but most studies show some variability in how well we achieve this.
Our attempts at accuracy are now helped by the availability of a surgical robot that helps with the planning and execution of the operation.
The most commonly used Robot in Australia is the MAKO* robot. This has been used for over 10 years in the USA but has been available in Australia for Partial knee replacements for 2 years, Total hip replacement for 1 year and is now available for total knee replacement as well.
Preoperatively the patient will have a CT scan which allows the surgeon the ability to plan the position of the component in all planes. During the operation the CT scan is matched to the patients’ anatomy, the bone is then prepared and the implants are positioned as per the plan.
Mr van Bavel performed the first Robotic Total Knee replacement in Victoria, as well as performing the first robotic total hip replacement and partial knee replacement at the Epworth hospital.
What equipment is used for a robotic operation.
The setup involves 3 separate pieces of equipment.

- A control area with screen and keyboard through which the plans are made and can be changed or updated at any stage.
- A sensor and screen that monitors the position of the leg and where the robot interacts.
- The robot and end effector ( tools).
- For a partial knee replacement this is a bur.
- For a hip replacement this is a reamer
- For a total knee replacement this is a saw.

What is Robotic partial knee replacement.
It is the replacement of a part of the knee with the assistance of a robot.
The Inner (medial), outer (lateral), front (patellofemoral) parts can all be replaced individually. Rarely a surgeon may want to replace 2 of the 3 parts at the same time ( Bicompartmental replacement).

How long has robotics been used to partial knee replacement.
The first Mako robotic partial knee replacement was performed in June 2006. Since then more than 50,000 procedures have been performed around the world. In Australia over 1000 procedures have been performed since its introduction in 2015. Mr van Bavel has been performing robotic Partial Knee replacements since 2016.
What is the revision (Redo) rate
In 2017 the Australian Orthopaedic Associations National Joint Replacement Registry showed a 1 year revision rate of the MAKO partial knee replacement to be 0.8% which is the lowest of all listed prosthesis. The average for all partial knee prosthesis was 2.2%..
This is in keeping with previously published data for the Mako from the USA showing a 1.0% 2 year revision rate.
There are is no long term data on survivorship of this procedure.
How is the operation planned.
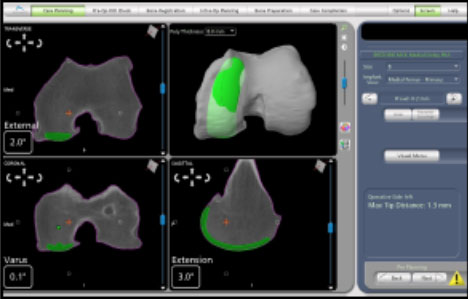
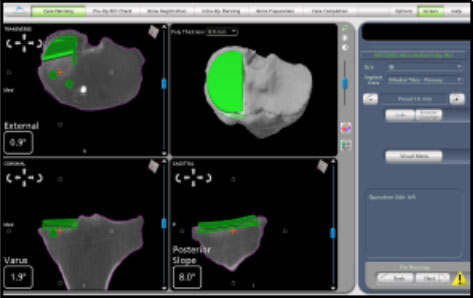
Prior to the operation the patient has a CT scan of the knee which allows the surgeon to plan the size and position of the implants that will be used during the operation. This allows matching of the implant to the patients’ personal anatomy.
How is the operation performed.
Small metal pins are attached to the leg and “trackers” or “arrays” will then tell the sensor where the leg is and when it is moved.

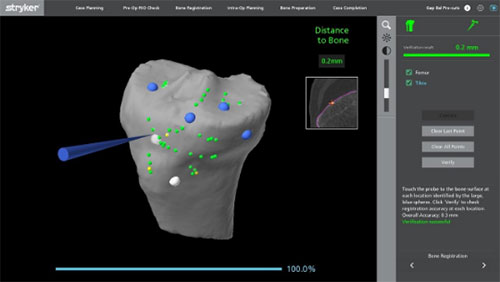
The patients’ anatomy is then checked and a series of points are registered to ensure the anatomy is matched to the CT scan.
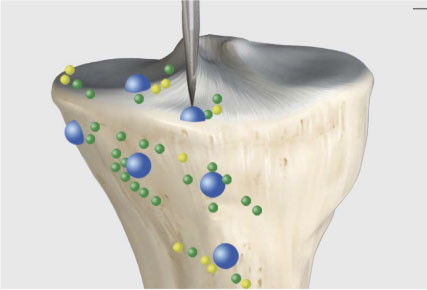
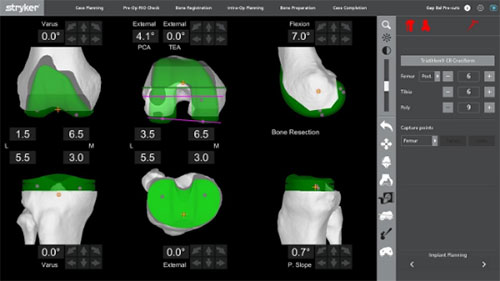
The knee is then put through a series of movements and the tension in the ligaments is measured and the movement of the knee is observed and the contact points between the components recorded. This produces a graph of the knee and a 3D model of how the knee will work after the replacement. The surgeon can then adjust the planned component position to change any aspect of the plan they want to improve.
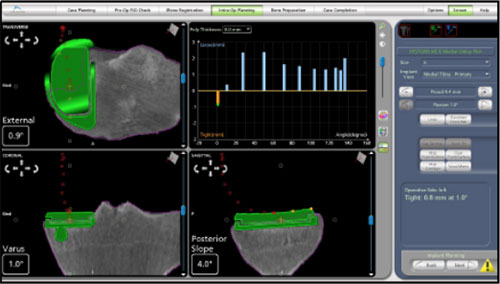
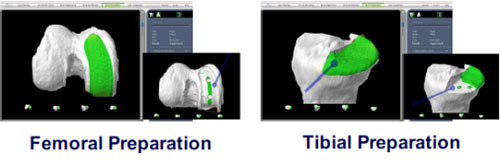
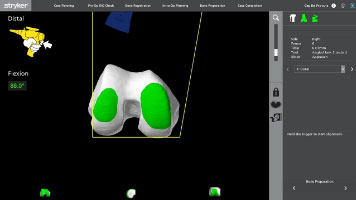
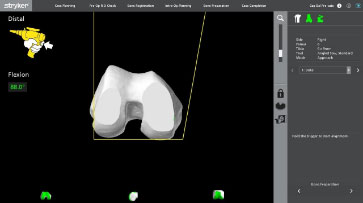
Once the plan is set the bone model is shown with an area highlighted in green which is the bone to be removed. The bur is then used by the surgeon to remove the bone but the robotic arm doesn’t allow the bur to move outside of the plan making this a highly accurate procedure.
Is this a “less invasive operation”
NO.
While the main cut used may be slightly smaller than a standard operation there is no significant difference in wound size.
What prosthesis is used.
The prosthesis used is called the “Restoris” partial knee replacement and was designed specifically for use with the Mako Robot.
Is it more accurate.
There have been studies which show improved accuracy using robotic for partial knee replacement. We hope that improved accuracy will lead to better outcomes for patients.
- Achieving accurate ligament balancing using robotic-assisted unicompartmental knee arthroplasty. Plate JF1, Mofidi A, Mannava S, Smith BP, Lang JE, Poehling GG, Conditt MA, Jinnah RH. Adv Orthop. 2013;2013:837167. doi: 10.1155/2013/837167. Epub 2013 Mar 24.
- Accuracy of Dynamic Tactile-Guided Unicompartmental Knee Arthroplasty, Dunbar, Nicholas J. et al. The Journal of Arthroplasty , Volume 27 , Issue 5 , 803 - 808.e1
- Improved Accuracy of Component Positioning with Robotic-Assisted Unicompartmental Knee Arthroplasty, Stuart W. Bell, Iain Anthony, Bryn Jones, Angus MacLean, Philip Rowe, Mark Blyth. J Bone Joint Surg Am Apr 2016, 98 (8) 627-635; DOI: 10.2106/JBJS.15.00664
- Yildirim G, Fernandez-Madrid I, Schwarzkopf R, Walker PS, Karia R. Comparison of robot surgery modular and total knee arthroplasty kinematics. J Knee Surg. 2014 Apr;27(2):157-63.
- In vivo kinematics of a robot-assisted uni- and multi-compartmental knee arthroplasty. Watanabe T1, Abbasi AZ, Conditt MA, Christopher J, Kreuzer S, Otto JK, Banks SA. J Orthop Sci. 2014 Jul;19(4):552-7. doi: 10.1007/s00776-014-0578-3. Epub 2014 May 2.
- Koskinen E1, Eskelinen A, Paavolainen P, Pulkkinen P, Remes V. Comparison of survival and cost-effectiveness between unicondylar arthroplasty and total knee arthroplasty in patients with primary osteoarthritis: a follow-up study of 50,493 knee replacements from the Finnish Arthroplasty Register. Acta Orthop. 2008 Aug;79(4):499-507.
- Short To Mid Term Survivorship Of Robotic-Arm Assisted Unicompartmental Knee Arthroplasty Thomas Coon, MD, Martin Roche, MD, Andrew Pearle, MD, Jon Dounchis, MD, Todd Borus, MD, Frederick Buechel, MD, Manoshi Bhowmik-Stoker, PhD, Michael Conditt, PhD 17th EFORT Congress 2016 Geneva, CH, 01-03 June
- Accuracy of UKA Implant Positioning and Early Clinical Outcomes in a RCT Comparing Robotic Assisted and Manual Surgery. Iain Anthony, Bryn Jones, Angus MacLean, Philip Rowe, Mark Blyth. University of Stracthclyde and Glasgow Royal Infirmary.
- Arno, S; Maffei; Walker, PS; Schwartzkopf, R; Desai, P; Steiner, GC. Retrospective Analysis of Total Knee Arthroplasty Cases for Visual, Histological and Clinical Eligibility of Unicompartmental Knee Arthroplasties. J. Arthorplasty. 2011. 26(8): 1396-1403
What is a robotic assisted hip replacement
It is an operation where the surgeon uses a robot during a hip replacement operation . This is the same as a normal hip replacement but a robot is used to try and get the components in an accurate position every time. We think that getting the hip replacement right is important for better outcomes for patients.
How long has robotics been used for hip replacement
The first robotic arm assisted hip replacement was performed in October 2010. In Australia the first Mako Hip replacement was performed in 2016. Mr van Bavel has been performing robotic hip replacements since February 2017.
How is the operation planned.
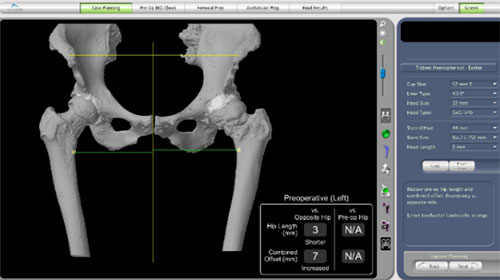
Prior to the operation the patient will have a CT scan of the hip. From this any difference in leg length between the 2 sides is measured and if necessary a correction can be made in the surgical plan. The size and position of the components is then planned to the patients’ own anatomy to try and get the best match for each patient.
Preoperative anatomy seen on CT scan
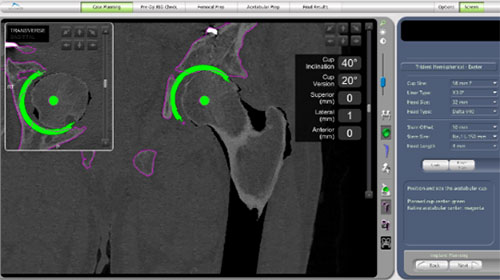
Planning the acetabular component position on the CT scan
The planned hip replacement with correction of anatomy to match the other side

How is the operation performed.
For the most part this is exactly the same as a standard hip replacement except for a few small differences. Metal pins are inserted into the iliac crest (pelvic bone) with an array attached which allows the robot to see where the pelvis is positioned at any time. Early in the surgery a series of anatomic landmarks around the hip are registered with the robot that allows it to recognize the anatomy and match it to the CT scan.
When preparing the bone for the acetabulum (socket) and inserting the prosthesis; instead of doing this freehand, the robot holds the instruments in the position that was planned to ensure the plan is followed. When preparing the femur the feedback from the robot informs the surgeon if what they are doing conforms to the original plan.

What prosthesis is used.
The prosthesis used for this are standard hip replacement prosthesis which have been around for many years. Mr van Bvael uses the Exeter/Trident hip replacement for this. This is the most commonly used hip replacement in Australia. It has excellent long term results.
What is the revision (redo) rate.
There is no data specifically looking at the redo rate for robotic hip replacement in Australia.
In The Australian Orthopaedic Association 2017 Annual Joint Replacement Registry the Exeter Trident hip replacement has a revision rate of 4.1% at 10 years and 5.7% at 15 years. The average revision rate for hip replacements in Australia is 6.6% at 10 years and 9.8% at 15 years.
Is this a “less invasive” procedure.
No. The same approach (cut) is used as a standard procedure. The robot can be used for any approach ( Posterior, anterior or lateral).
Is it more accurate ?
There are some early research papers that show increased accuracy of component positioning with robotics compared to manual techniques. We hope this will lead to a lower dislocation rate and better patient outcomes.
- Nawabi DH;Conditt MA; Ranawat AS; Dunbar NJ; Jones, J; Banks S, Padgett DE. Haptically guided robotic technology in total hip arthroscopy - A cadaveric investigation. Journal of Engineering in Medicine. December 2012. [Epub ahead of print]
- Dounchis J, Elson L, Bragdon C, Padgett DE, Marchand R, Illgen R, Malchau H. A Multicenter Evaluation of Acetabular Cup Positioning in Robotic-Assisted Total Hip Arthroscopy. 43rd Annual Course: Advances in Arthroscopy, October 22-25, 2013, Boston, MA
- Domb BG, EL Bitar YF, Sadik BS, Stake CE, Botser IB. Comparison of Robotic-assisted and Conventional Acetabular Cup Placement in THA: A Matched-Pair Controlled Study. Clin Orthop Relat Res. 2014 Jan;472(1):329-36
- Domb BG, et al,. Does Robotic-Assisted Computer-Navigation Affect Acetabular Cup Positioning in Total Hip Arthroplasty in the Obese Patient? A Comparison Study. 14th Annual CAOS Meeting, June 18-21, 2014, Milan, IT.
- Domb BG, et al,. The Learning Curve Associated with Robotic-Assisted Total Hip Arthroplasty 14th Annual CAOS Meeting, June 18-21, 2014, Milan, IT.
- Illgen R. Robotic Arm Assisted THA Improved Accuracy, Reproducibility and Outcomes Compared to Conventional Technique. 43rd Annual Course: Advances in Arthroplasty, October 22-25, 2013, Boston, MA
- Accuracy of Cup Positioning and Achieving Desired Hip Length and Offset Following Robotic THA. Jerabek SA; Carroll KM; Maratt JD; Mayman DJ; Padgett DE; 14th Annual CAOS Meeting, June 18-21, 2014, Milan, Italy.
- Efficient and Accurate Hip Length and Combined Offset with the MAKOplasty THA Femoral Express Workflow, Thompson, M., March 2014
- Bukowski, B.; Abiola, R; Illgen R. Outcomes after primary total hip arthroplasty: Manual compared with robotic assisted techniques. ; 44th Annual Advances in Arthroplasty; Cambridge, MA. October 7-10 2014.
- Suarez-Ahedo, C; Gui, C; Martin, T; Stake, C; Chandrasekaran, S; Christopher, J; Domb, B. Preservation of Acetabular Bone Stock in Total Hip Arthroplasty Using Conventional vs. Robotic Techniques: A Matched-Pair Controlled Study. CAOS International 15th Annual Conference; June 17-20, 2015, Vancouver, Canada.
What is robotic assisted knee replacement
It is a knee replacement where the surgeon utilizes a robot to help with the operation
How long has robotics been used for knee replacement
The first robotic arm assisted Total Knee replacement was performed in June 2016. Mr van Bavel performed the first Robotic knee replacement in Victoria in November 2017. Mr van Bavel is one of the national Trainers for MAKO robotic Knee replacement surgery. Due to the advantages of robotic surgery Mr van Bavel performs all of his knee replacements with the MAKO robot.
How is the operation planned
Before the operation the patient will have a CT scan of the knee. From this the size and positioning of the prosthesis is planned to fit the patients anatomy.
How is the operation performed.
The operation is very similar to a standard knee operation and uses the same cut at the front of the knee. 2 small pins are attached to bone on either side of the knee and this helps the robot during the operation. Early in the operation multiple landmarks are checked and rechecked to allow matching of the patients anatomy to their scans.
After assessing the patient’s ligament tension, gap analysis, and limb alignment, surgeon controlled intra-operative adjustments can be made to the pre-operative plan in both flexion and extension before bone preparation.
Ie The plan is then checked and adjusted with the surgeon aiming to give the best knee replacement - ie one that moves well , without pain and feels as close to normal as possible..
The robotic arm then controls the saw blade as the surgeon cuts the bone in the planned position. The total knee application creates a stereotactic boundary which assists the surgeon in executing both the tibial and femoral bone resections to plan. The stereotactic boundary has the potential to protect essential anatomical structures of the knee during bone preparation including the PCL and the popliteal artery


What prosthesis is used
The Triathlon Total Knee system from Stryker. This is the most commonly used knee replacement in Australia.
What is the revision (redo) rate.
In 2021 the AOA National Joint Replacement Registry showed a slightly lower revision rate for Robotic knee replacement compared to knee replacement performed manually. The procedure uses the Triathlon knee replacement and there is abundant long term data on its success.
According to the 2017 AOA National Joint Replacement Registry the Triathlon Cr has a 3.2 - 3.9% 10 year revision rate. The average revision rate across Australia for all knee replacements is 5.3%. Due to this the triathlon has been awarded a 10 year superiority benchmark
Is this a “less invasive” procedure.
A very similar size cut is used to a standard procedure. Some studies have shown less soft tissue damage with robotic surgery. this may contribute top less pain, better range of motion and an easier recovery.1
Is it more accurate ?
There have been a couple of research papers 2,3 looking at this which show increased accuracy and precision, and protection of the soft tissues around the knee. Increased accuracy allows a more customised plan to better fit individuals bone anatomy and biomechanics
What do we do to make your recovery better – how can we improve the patient Journey.
We have tried to streamline our processes to make it quicker and easier for you to have your knee replaced. We have a dedicated preadmission clinic where you will be seen by our peri-operative physician who ensures you are in peak health for your operation. Our physiotherapist will show you some exercises to help get you in shape and give you some advice to set you on your way to recovery. All of your preop scans will be performed at the time of your pre admission clinic.
During your surgery your knee joint and the tissues around it will be infiltrated with local anaesthetic to help minimise your pain, this is part of the multimodal analgesic regime. This will be topped up for the 1st 24 hours after surgery. Our patients often use a perio-operative app that will also help guide you through the process of surgery and recovery, it will show you exercises and will help document your recovery.
Does it work ?
Please read the reviews on these independent website.
https://www.doctoralia.com.au/files/dirk-van-bavel/orthopaedist/hawthorn-east/
https://nicelocal.com.au/melbourne/medical/dirk_van_bavel-5348/
or look at our google reviews
To Book an appointment with Mr van Bavel call 03 9882 7753
1 Kayani B, Konan S, Tahmassebi J, Pietrzak JRT, Haddad FS. Robotic-arm assisted total knee arthroplasty is associated with improved early functional recovery and reduced time to hospital discharge compared with conventional jig-based total knee arthroplasty: a prospective cohort study. Bone Joint J. 2018 Jul;100-B(7):930-937.
2 Robotic-Arm Assisted Total Knee Arthroplasty Demonstrated Accuracy To Plan Even During Learning Phase Hampp E., Scholl L., Prieto M., Chang T., Abbasi A., Bhowmik-Stoker M., Otto J., Jacofsky D.J., Mont M.A. European Knee Society Arthroplasty Congress 2017, London, UK, 20 & 21 April 2017
3 Robotic-Arm Assisted Total Knee Arthroplasty Demonstrated Soft Tissue Protection Hampp E., Bhowmik-Stoker M., Scholl L., Otto J., Jacofsky D.J., Mont M.A. European Knee Society Arthroplasty Congress 2017, London, UK, 20 & 21 April 2017


